 Whatsapp
Whatsapp
 Call Now
Call Now


Prosthetic Eye

Congenital Microphthalmia – Anophthalmia
It can be defined as underdevelopment (microphthalmia) or undevelopment (anophthalmia) of one eye or both eyes in the womb. This condition can be caused by various infections, genetic factors or medications used during pregnancy, or it can be an isolated case with no known cause.
Our priority in these patients is to investigate the possibility of vision in that eye or eyes, and then to plan the cosmetic correction of the

external appearance so that the child is accepted and not ostracized by other individuals and therefore does not have psychological problems.
The absence of a healthy growing eye in the eye socket reduces the stimulation of the bone and soft tissues around the eye, resulting in a smaller and flattened appearance in these tissues compared to the other healthy side. If this condition is bilateral, an “hourglass” looking head and face may appear as a result of the upper and lower sides of the head developing and the eye area remaining narrow.
It is very important to start treatment immediately in order to ensure that such children are integrated into society as healthy individuals and are not ostracized by other children.
The eye development problem in each patient may be different. After the level of eye development retardation in the child is determined by an experienced oculoplastic surgeon, a patient-specific treatment plan should be created.
These treatments are decided entirely according to the patient’s eye condition and cover a wide range from conformers to be placed in the eye socket without any surgical intervention and enlarged over time, to space occupiers to be placed in the eye socket with various numbers of surgeries (orbital implant, sphere, dermis-fat graft).
The important thing here is to start treatment with appropriate specialists and under appropriate conditions without wasting time. The aim of these treatments is to make the child able to wear prosthesis until the preschool period and to provide an appearance that is not very noticeable from the outside.
Evisceration – Enucleation
Complete removal of the eyeball for various reasons is called “enucleation”, while removal of only the inner part of the eyeball, leaving the outer white tissue (sclera), is called “evisceration”. While enucleation is mostly preferred in the presence of intraocular tumors, evisceration surgery is preferred for reasons such as infection, shrinkage of the eye after trauma.
In both surgeries, permanent space occupiers (orbital implants, spheres) are placed in the eye socket to compensate for the lack of volume caused by the removed or evacuated eyeball. After enucleation surgery, the muscles that move the eye are attached either to the surrounding soft tissues or to the implant.
In evisceration surgery, the implant placed inside the sclera can be moved by the muscles since the scleral tissue to which the muscles are attached is not removed. In this way, the movement of the prosthesis to be inserted from the outside is ensured.
Orbital implants placed in the eye socket during surgery are made of different materials. Orbital implants can be classified into porous implants (natural coral or bioceramic hydroxyapatite), which allow blood vessels in the body to penetrate and thus integrate into the body, and non-porous implants made of acrylic or silicone.
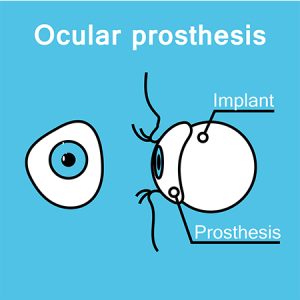
Prosthetic Eye Application
The prosthesis can be applied in front of the patient’s own eye (scleral shell), which is blind, smaller than the other eye and cosmetically unsightly from the outside, or after evisceration or enucleation surgery when this is not possible due to sensitivity or disease of the eye.
Except in cases that require surgery, such as severe eye sensitivity, open trauma or tumor, the prosthesis can be first tried on the patient’s own eye. After this trial, patients who are comfortable with the prosthesis can wear a prosthetic eye without surgery. In patients who cannot tolerate this, the eye socket is prepared for the prosthetic eye by surgically removing sensitive tissues (evisceration).
Prosthetic eyes can be purchased and used ready-made, or they can be molded in prosthesis laboratories and produced individually. In suitable patients who can wear prosthesis without surgery, molds can be taken for prosthesis and prosthesis making can be started immediately, while in patients who have undergone surgery, it takes approximately 6-8 weeks for the socket to be ready for prosthesis making. At the end of this period, prosthesis can be started in patients with a suitable socket.
After the start of prosthesis use, the prosthesis should not be removed from the eye socket except for prosthesis cleaning, and you should not sleep without the prosthesis at night. It is recommended to remove and clean it once a week. Otherwise, problems such as socket narrowing, inability to wear the prosthesis afterwards, and severe burrs as a result of infection may be observed.

Socket and Implant Problems
Whether the eye socket in which the prosthesis is inserted is surgically created or a prosthesis (scleral shell) is placed on a shrunken eye, the prosthesis is inserted into the eye socket (socket) covered by the conjunctiva, the outer membrane of the eye. Problems may occur in the socket as a result of improper prosthesis use or various external factors.
As a result of these problems, narrowing of the socket and the inability to wear the prosthesis may occur. Patients who can no longer wear the prosthesis as comfortably as before should be examined by an experienced oculoplastic surgeon without wasting time and the origin of the problem should be determined. If there is a narrowing of the socket as a result of the examination, it should be planned to repair the missing tissue with the most suitable tissue, such as conjunctiva of the other eye, oral mucosa or amniotic membrane.
Another problem that may occur after evisceration or enucleation surgeries for prosthesis placement is the expulsion of the implant. Although the orbital implants used during these surgeries are made of materials that the body will not reject, these implants may be expelled over time.
In such a case, the cause should be thoroughly investigated, these implants should be removed from the body as soon as possible and if possible, a suitable implant or dermis-fat graft from another part of the body should be placed in the same session.
The eye socket should not be left without an implant as much as possible, as there is a possibility of serious volume deficiency in unimplanted sockets and as a result, larger prosthesis to complete that deficiency and then there may be bigger problems with the prosthesis.
After these socket surgeries, healing should be expected to be completed (approximately 6-8 weeks) and then either the prosthesis should be modified or the prosthesis should be reproduced due to changes in the prosthesis socket.
Prosthetic Eye Prices 2024
You can contact us to get information about Prosthetic Eye Prices 2024.